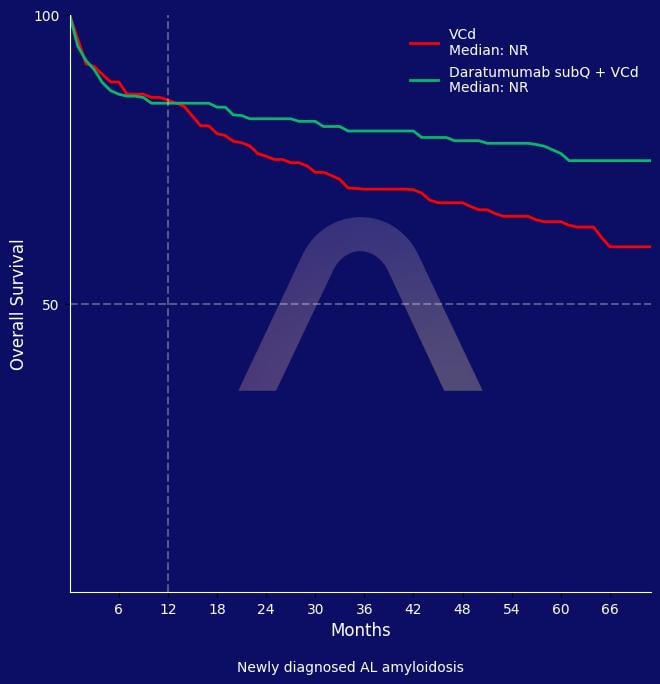
In this phase 3 trial of newly diagnosed AL amyloidosis, adding subcutaneous daratumumab to VCd significantly improved hematologic complete response rate. The combination also improved cardiac and renal responses, major organ deterioration–progression-free survival. Overall survival was numerically improved with addition of daratumumab. Safety profiles were consistent with known effects, with manageable adverse events supporting D-VCd as the new standard of care.
Study
|
Randomized, open-label, phase 3 study [ANDROMEDA] |
| Newly diagnosed AL amyloidosis |
| Six cycles of VCd alone (n=193) vs VCd plus subQ daratumumab (D-VCd) followed by daratumumab maintenance x 2 yrs (n=195)
|
Efficacy
|
Hematological CR: 59.5% vs 19.2% (D-VCd vs. VCd) (OR 6.03 [3.80-9.58]) |
| Cardiac response: 65% vs 32% |
| Renal response: 54% vs 27% |
| Median major organ deterioration–PFS: NR vs. 30.2 mos (HR 0.44 [0.31-0.63]) |
| Overall survival: HR 0.62 [0.42-0.90] |
| 5-yr OS: 76.1% vs 64.7% (HR: 0.82 [0.50-1.35])
|
Safety
|
Grade 3 or above AEs: Lymphopenia (13.0% vs 10.1%), pneumonia (8.3% vs 4.3%), diarrhea (6% vs 4%), cardiac failure (6.2% vs 2.7%), neutropenia (5.2% vs 2.7%), syncope (6.2% vs 6.4%), fatigue (5.2% vs 3.2%) |
| Peripheral sensory neuropathy grade >=2 (13.5% vs 9.6%) |
| Treatment discontinuation due to AEs: 5.2% vs 4.3% |
| Deaths due to AEs within 30 days: 11.4% vs 7.4%
|
Blood. Published online May 12, 2026
http://doi.org/10.1182/blood.2025032099
Reviewed by Ulas D. Bayraktar, MD on May 14, 2026